
Publisher:
Bonnie King
CONTACT:
Newsroom@Salem-news.com
Advertising:
Adsales@Salem-news.com

~Truth~
~Justice~
~Peace~
TJP
Sep-08-2012 15:03

 TweetFollow @OregonNews
TweetFollow @OregonNews
Controlling Opium
M. Dennis Paul, Ph.D. Salem-News.comWhen Reason and Rationality Are Trampled By Politics and Emotion
 Courtesy: southasiaspeaks.wordpress.com |
(WINDSOR, N.H.) - “He sat in the courtyard watching his children spinning and spinning, their arms flailing as they cut through the air with each turn. Such giddiness and uproarious laughter had never before been witnessed, by him, in his children. Even when they fell to the earth bumping their knees and elbows, the looks of pure joy coupled with moans and laughter puzzled him. Within a minute or two, the children would bolt upright and begin this curious dance once again and the laughter and glee continued as such for some time. Relighting his prized cigar, he then sipped on the rare, fragrant whiskey his brother had sent from Ireland, felt its golden warmth fall through his body and the delightful tinge of relaxation walk across his brow, placed his glass down on the arm of his chair and continued observation of his children at play while circles of smoke lofted above him in the gentle breeze.”
The above is an excerpt from the opening of a lecture to Psychology students given in 1999. In one paragraph, the history of man's quest for another “reality” is exposed. The quest for a sense of self outside of the every day awareness of self is, perhaps, one of the most natural quests of man. From the sensation of dizziness with its inherent tricks of making one feel lighter than air and then suddenly heavier than stone all the while stimulating pleasure zones wired into our brains, this quest is clearly demonstrated to exist within us from very early ages. As we age, there appears to be no less a desire to experience a reality other than what exists in what we call our “normal” state.
For some, whether early on or later, this quest takes on an urgency carrying it beyond the simple desire of experience. For some, it is a quest to hide from fears and anxieties that may accumulate from both an unpleasant environment and/or a confused internal dialogue which constantly “reminds” us that the world is not conforming to what we demand. It is not the picture of the world implanted within over years or the one we dream but which disappears every time we open our eyes.
Here, we begin to differentiate the human who seeks an experience of a different reality from the human who seeks to medicate away reality. It is not so simply black or white, however. Within exists the human who “moderates” reality for himself. This human seeks both medication to ease the stressors of daily living and, perhaps, an occasional break from moderation and self control. Some may only seek an occasional break from daily exercise of control. These are but a few of the known variations.
Scientists and doctors have labored for many years to explain why some humans can abstain or self moderate while others cannot. In the past 30 or so years, frustrated yet arrogant researchers have decreed that, without a single shred of evidence, those who are unable to moderate or abstain are afflicted with a medical disease. The term “addiction” now becomes something completely out of the hands of the individual and places it amongst the medical problems of bacterium and virii which they then seek to destroy with chemical nostrums.
In recent years, unable to find or create a nostrum which effectively crushes “addiction”, the wise men from Harvard decreed that ALL “addicts” suffer a dual diagnosis...which is to say that they also have a mental disease on top of their “addiction”. The thinking was that if doctors (primarily of Psychiatry) could get a chemical control upon the mental disease of the “addict”, the second disease, that of “addiction” could be more readily “cured”. However, those of us who have worked in the “addiction” field saw first hand how well (sarcasm) this actually worked as our clients began to come to detox facilities inebriated and with a bag full of neuroleptic medications... some of which are actually harder to detox from than the DOC (Drug Of Choice) of the client and are, in some cases, far more injurious and even deadly than their DOC. As someone who was assigned to a clinical “Dual Diagnosis” team, I was witness to some of the most deranged clinical arguments regarding the rationale and efficacy of such diagnoses.
Irrational arguments abound in every arena of life. Most are drawn from emotionality and politics. Most are supported by cognitive distortion and personal, as well, group induced bias. None of these arguments ever effectively addresses whatever issue is in contest. What occurs, is lines being drawn, detrimental legislation being proposed, and harm heaped upon those most in need of help.
One issue which remains a constant in the pages of Salem-News is the battle for control over the prescription of Opioids. It is not my intent, nor any desire, to disparage contributors to Salem-News who have positioned themselves in what I consider to be detrimental journalistic endeavor. The primary writer addressing this issue is, I can assure you, someone of unquestionably good character who genuinely cares about this issue.
My intention is to hopefully explain to this writer and her followers, and to all the readers of Salem-News, why these propositions, and the reasoning behind them, are inherently flawed, misguided and harmful.
In the above paragraphs I attempted to give a brief view of man's nature and desire to explore, use, or abuse various mind altering substances. Too, a brief view of how such presentations are externally viewed. To continue with my argument, it becomes necessary to address in a bit more detail the history of Opioids and Opioid use and/or abuse. In so doing, I hope to impart a greater understanding of what “addiction” entails and how the term is so inappropriately applied.
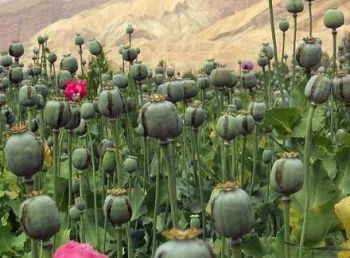
Opium, the latex extract from the pod of the Poppy plant (Somniferum var.) has been used both medicinally and recreationally since before historical records. The oldest known presence of the Poppy resides in findings from the Neolithic era. The oldest known use of Opium stems from the Sumarians in approximately 3500 BC (roughly 5500 years ago) in the region now known as Iraq. While records indicate that its use was medicinal, its name implies a bit more. Opium in Sumaria was called hul gil which means “joy plant”. Sumarians were known to be large growers of Opium as well producers of a much desired beer. In fact, estimates are that over half of their barley crop was used for production of beer. Opium, beer, and a variety of foods were the major exports of Sumaria. Surprisingly, there exists little record of societal degradation, disease and death from Opium during this period.
By 1300 BC, Egyptians were were producing Opium and exporting it to areas of Greece and also central Europe. Again, use was both medicinal and recreational. Again, little indication of societal degradation. The first known mention of Opium by the Greeks was Hippocrates around 330 BC. Around 150 BC another doctor, Galen, describes what is, perhaps, the first recorded overdose on Opium. He continued to advocate for its use, however. Advocacy for Opium, in Greece, continued into the 1st century AD. Today, while illegal, old farmers in both Greece and Turkey produce a liqueur, Ouzo (now commercially made as a wine and absent two key ingredients), made with both Absinthe and Opium. As a child of 10, I was fortunate to have been given a taste of this “mountain” made elixer and can attest to the clean and exquisite flavor as well the remarkable “sensations” it imparts.
Alexander the Great re-introduced Opium to Persia around 330BC. The Sumarians had once traded with Persia but as the Sumarians disappeared, so did their Opium and it was forgotten. About 700 years later, Opium was introduced to China. This was Egyptian Opium brought to China by Arab traders for whom Opium was a major trade product. Images of Chinese people smoking Opium have given many the impression that this was the normal method for using Opium. This, however, is not so. For the better part of history, Opium was consumed as a liquid. Smoking opium came much later and was actually, to the best of our knowledge, introduced by Dutch traders who enjoyed mixing Opium with tobacco. It was around 1700 AD that the practice of smoking Opium came to China via Portuguese traders. The Chinese quickly gave this up for the method of direct vaporization and this remains the most popular form of use today.
In the early 1500's, a tincture of Opium became popularized. This was called Laudanum and was the favored intoxicant of famed writer Edgar Allen Poe who died in 1849 which attests to the continued use of this product over roughly 4 centuries. Laudanum is, in fact, still available today. Back in the 1500's, however, while numerous additives were used, one of the most sought after concoctions was Sydenham's Laudanum, which was a combination of sherry and opium. Sydenham's Laudanum was, in fact, the first known “Patent” medicine.
Throughout most of history, the trade in Opium was simply trade. Opium was a commodity much sought after both for its medicinal qualities, which are indisputable, and for its recreational use... also indisputable. In the late 1600's and into the 1700's, trade in Opium became political. Nations such as England, Portugal and the Netherlands began to encroach upon each others trade, particularly with China who had, for various reasons, difficulty in producing its own Opium. By 1800, England came out on top in trade with China through the East India Company who had become deeply entrenched within the government of England.
Europeans desired numerous commodities from China (the British primarily desiring the skillfully crafted teas of China) but the Chinese desired very little, aside from Opium, from Europe. Eventually, a trade deficit occurred which began to unsettle China. Shortly before 1796, China outlawed smoking of Opium. This was the beginning of an effort to reduce demand which would, it was supposed, begin to resolve the growing trade deficit. Village elders began scare programs warning citizens that Opium would shrivel their faces and similar such tactics. In 1796, China banned all trade in Opium and resolved to make due with its own inferior and not so abundant Opium. For the next 40 years, these laws were rarely enforced. Once the Chinese government decided to actually attempt enforcing these laws, the “Opium Wars” broke out. In reality, while it is claimed there were two “Opium Wars”, there was really only one with a cease fire of some length in between.
We have been “taught” that these wars were between a caring Chinese government vehemently attempting to save its population from the ravages of Opium addiction and the English government hell bent on enslaving the Chinese by any means...Opium being the most effective. As I stated prior, the reality was the trade deficit. China still wanted Opium and the stated cause of the wars was, in reality, theft of Opium from the British, not the British trying to force the Chinese to buy more Opium. The Chinese wanted the Opium and the British wanted to sell it to them. Prices and the growing trade deficit produced these wars (war).
China was not plagued by a mass epidemic of crazed Opium “addicts”. Proof of this lies in the conservation habits demonstrated by the Chinese during periods of price increases. When England purposely limited export of Opium to China, causing price increase, the Chinese people bought less Opium and made it last longer. When India produced Opium (the British product) became scarce, China was fine dipping into its own inferior product as well as obtaining small amounts from other countries.
Iranians, considered to be the largest modern day consumers of Opium, again demonstrate the lack of crazed Opium addicts. When the Taliban outlawed production of Opium (it was never completely halted although production was seriously curtailed), Iranians, rather than becoming a mass of hysterical withdrawing addicts, immediately substituted Opium with Hashish. Not only did the Hashish help them get through the actual withdrawal from Opium (much milder than that from Heroin and Methadone) it satisfied their want for an alternate reality. From what we know of their existence, who could blame them. What Opium did enter Iran during that period was made to last longer through moderation. Of course, greedy bastards also began to import Heroin into Iran and this was rather severely cut with any number of additives. Primarily, city youth preferred Heroin as it was cheaper, smaller amounts were needed to get high, and it was much easier to conceal. The older Opium smokers preferred to stick with Hashish and the small amounts of smoke-able Opium they could obtain.
Iran, historically, was not concerned with Opium use as it presented no societal degradation. It was not until the US began a program of introducing Heroin and other drugs (cocaine, methamphetamine, etc) into Iran and also began exporting its views on addiction, interdiction and treatment that Iran began to attack Opium use.
In the US, Opium once flourished widely. This came to a halt in the early part of the 20th century and was due, in large part to the US wanting to trade with China. Surprisingly (or not, depending on your political acumen) the first laws against Opium in the US were directed at the Chinese. Whites remained exempt. I won't delve into the Eugenics movement of that period which played a tremendous role in the global program of outlawing recreational drugs. To do so, here, would take away from my initial intent. Suffice to say that racism plays an enormous part in the institution of drug laws and the rationale for such laws has been cloaked in both improperly conducted and promoted “science” and emotionality generated to scare people from having their faces shriveled.
I will, in mentioning “science”, direct readers to an oft cited “study” which when abstracted in various media paints a very dire empirical dogma regarding death and disease ostensibly caused by Opium use. In this“abstract” http://6ci.jy.sl.pt the imposition of absolutism could not be more blatant. However, in this “abstract” of the very same study note this following passage: "Based on the overall adjusted hazard ratio for opium use of 1.86 (1.68 to 2.06), and assuming this represents a causal association, we calculate the fraction of deaths attributable to opium in this population as 14.9% (95% CI 2.3 to 17.5)," Malekzadeh and colleagues wrote.
They noted that the possibility of reverse causality and confounding existed because of the observational nature of the study. An additional limitation of the study was from use of "verbal autopsy" from physicians rather than postmortem examinations, according to the investigators.
This represents a “study” which is actually a monumental leap away from true science and is, in fact, evidence of only the initial bias of its authors. ( Khademi H, et al "Opium use and mortality in Golestan Cohort Study: prospective cohort study of 50,000 adults in Iran" BMJ 2012; DOI: 10.1136/bmj.e2502.)
If one takes the time to read the actual “study”, the errors and omissions as well as the incredible leap from the precipice of reality becomes ever more apparent.
You might ask why I highlight this study. Two very important reasons. One, it is highly representative of the types of research conducted today with regard to most any drug and, two, inept and/or purposely biased individuals tend to take such “studies” to even greater leaps of reality... such as the following:
In an editorial accompanying the article, Irfan A. Dhalla, MD, of St. Michael's Hospital in Toronto, noted that clinicians in developed countries are unlikely to ever see a patient who uses opium.
However, millions with chronic noncancer pain use opioid medications such as morphine, codeine, and oxycodone.
"Are these patients, like opium users, also at increased risk of death?" asked Dhalla.
The risks of opioid drugs are "incompletely understood," he noted, adding that "for the management of chronic noncancer pain, a better prescription may be caution."
Can DR. Dhalla not see the obvious failure of this “study” to produce any rational result?
One of the greatest hysterias promoted regarding use of opioids is its supposed epidemic status in the US. Taking a look at historical figures for Opium use in any given population results in figures along the line of 2.7% to a maximum of 3.4% of said populations using Opium. The figures for “addiction” typically reflect a lesser number as it is understood that not all users are “addicts” (despite what some might hope you will believe). So let's take a look at prescription Opioid use (as well as non-prescription use which is all too often ignored when individuals and groups attempt to politicize and emotionalize the issue) in the US. From Harvard Medical Publications dated 2011 (http://6cj.vj.sl.pt ):
The issue of painkiller addiction is receiving more attention because prescriptions for opioids have increased tenfold since 1990. Paralleling this trend, the number of people addicted to painkillers has also increased over time.
Columbia University researchers found that opioid addiction had tripled over a 10-year period, with the proportion of Americans reporting abuse or dependence increasing from 0.1% of the population in 1991–92 to 0.3% in 2001–02. The 2009 National Survey on Drug Use and Health found that nearly two million Americans were dependent on or abusing prescription pain relievers — nearly twice as great as the number of people addicted to cocaine.
Please note that a false accumulation of data occurs when “abuse” is lumped in with “dependence”. Also note that the reference to the year 2009 fails to denote a percentage of the population. This omission is not without intention. To continue:
According to the latest statistics compiled by the Centers for Disease Control and Prevention, in 2007 painkillers killed twice as many people as cocaine and five times as many as heroin. Opioid painkiller addiction was also more common than abuse of or dependence on any other type of prescription drug.
Several things can be implied by such a statement. Being that Opioids are twice as prevalent as cocaine, 2 times the amount of Opioid attributed deaths occur as a result of their use. (False) Opioids are more deadly than cocaine. (False) Heroin is five times less deadly than other opioids. (False) Truthfully, whatever assumption one makes from such a comment will result in an incorrect assumption. This represents the skewed nature of research and interpretation prevalent in science and medicine. This represents a complete failure of science and an intentionally biased outlook on Opioids (in this case).
Another fallacy and all too often promoted idea is the actual deaths and death rates attributed to Opioids. There are actually no known studies which clearly separate causes of death where multiple drugs (including alcohol) as well as other underlying or concomitant issues exist. None. I have been reading the literature for well over 20 years and have yet to find one. When challenged, others offer one after another which invariably fail... and often in more ways than any rational scientist would ever be able, honestly, to overlook. In most all deaths attributed to Opioids, the concomitant factors are considerable. Among these are benzodiazepenes which are commonly prescribed (and sought after) by abusers and “addicts”. Benzo's have their own high risk factors for mortality as they also slow the rate of respiration.
From the CDC weekly Morbidity and Mortality Report ( http://6cj.zx.sl.pt) Feb. 17, 2012
In 2008, a total of 36,450 drug overdose deaths (i.e., unintentional, intentional [suicide or homicide], or undetermined intent) were reported, with prescription opioid analgesics (e.g., oxycodone, hydrocodone, and methadone), cocaine, and heroin the drugs most commonly involved (1).
Since the mid-1990s, community-based programs have offered opioid overdose prevention services to persons who use drugs, their families and friends, and service providers. Since 1996, an increasing number of these programs have provided the opioid antagonist naloxone hydrochloride, the treatment of choice to reverse the potentially fatal respiratory depression caused by overdose of heroin and other opioids (2). Naloxone has no effect on non-opioid overdoses (e.g., cocaine, benzodiazepines, or alcohol)
Note that this figure represents prescription drugs as well illegal street drugs of unknown quality and composition. Note also that Benzo's are included along with alcohol and cocaine but other drugs are not mentioned despite their use on the street in conjunction with those drugs listed. Note further, that this report fails to mention that nearly 1/3 (a number which has remained fairly static for many years but appears to be decreasing) of overdose deaths occur in individuals who use methadone as their primary drug. This figure represents those prescribed methadone for pain as opposed to Heroin users on maintenance treatment. The dangerous use of aluminum foil in smoking opioids is never mentioned although it is one of the most common practices for opioid users.
CBS NEWS JULY 4, 2012 (CBS News) Methadone accounts for only 2 percent of painkiller prescriptions in the United States - but the drug is behind more than 30 percent of prescription painkiller overdose deaths, the Centers for Disease Control and Prevention announced Tuesday.
Surprisingly (or not, depending on your political and medical acumen), programs in many regions of the US and in other nations are realizing that heroin is both safer and more cost effective in treating addicts. In other words, it is better to clinically administer heroin to those in need than to maintain them with methadone, benzo's and the like.
Here, we need to discuss the actual reporting of causality for death. The reported number of deaths from opioid analgesics in the year 2009 was approximately 16000 although the agencies involved claim this is underestimated as reporting came prior to final statements regarding some deaths. When questioned on how these figures are determined, the various coroners I have confronted over the years will say that they report based on the presence of an opioid in the system at time of death. Some add that they also include method of death... usually respiratory failure. Almost all of them reported little or no concern that several other respiratory inhibiting drugs, including alcohol and tobacco, benzo's of all sorts and a host of others were present at the time of death. This represents a gross bias toward reporting opioids as cause of mortality. Further, these reportings and resultant figures fail to provide information regarding intention of the user or source of the drugs used. These are left up to studies which, based on already biased reporting of cause for death are necessarily further biased.
Another study now frequently used in arguing against opioid treatment for non-cancer pain is http://www.
I am truly surprised that these authors are allowed to get away with such sloppy work. And this in spite of the knowledge that better than 90% of all studies today that pass as science are based on thin or non existing air. “Publish or Perish” is the curse of modern science and medicine.
Most individuals have no idea how the term “non-cancer” pain came to be the prevalent criteria for both discussion and prescription of opioid analgesics. It's actually rather simple. Years ago, there existed a struggle to justify use of continued and high dose opioid treatment for chronic cancer patients. After considerable struggle, it became a common theme (and practice) that it was humane to allow such treatment for these clients due both to the degree of pain they experience and the presumed inevitability of their demise. There is, however, not a single scientific study which establishes this rationale. Not one. Further, if one examines the McGill (University) pain scale ( http://6ck.gg.sl.pt), chronic cancer pain is actually far less than that of other long term and incurable conditions. I know this to be a fact because I am one of many individuals who must live with what is known to be the most painful of all conditions.
Today, despite knowledge that more and more cancers are being effectively treated and reversed, despite knowledge that there are chronic conditions far more painful than chronic cancer, and despite the complete absence of any scientific research showing it is more humane and compassionate to allow long term opioid use for chronic cancer than for conditions far more painful and disabling...even deadly, the so-called researchers and proponents of irrational controls over opioid prescribing continue to use this vacant term to impress readers of something.. perhaps their compassion?
I am very clear in my position that there exists a very humane rationale for prescribing long term opioid therapy for those who suffer as much as I have for over 20 years. I am clear that short term pain relief where indicated is also humane. I bit the bullet for 17 years refusing to use opioids. I am not unrealistic in recognizing that such therapy has its drawbacks. My condition took a dramatic turn for the worse a few years ago and I had no choice. My life was hell for 17 years and there is no way to adequately infuse that reality into anyone else 's thinking. It has to be experienced for one to truly understand. Some letter to the editor doctors have attacked me claiming that I hadn't tried alternative pain treatment methods. They don't know me but somehow felt they could determine this as fact. They were very wrong. To be fair, I was also attacked by religiously invested hypnotists. I used hypnotherapy for almost 17 years being that I am a highly trained hypnotherapist and educator.
Those who promote legislation such as the so called citizen's petition http://www.citizen.org/
I'm not going to go through each and every citation in this non-citizen petition as this would become tedious for the reader, however, suffice to say that the very first of their citations utterly fails to support their use of it inside their petition. Morbidity and Mortality Reports all too often fail to support their own conclusions as they provide more confounding data than is rationally and scientifically feasible for much of any conclusion to be drawn. They also make recommendations that are too often beyond any reason.
In this particular report, one recommendation is that prescribing of pain medication should be determined and controlled in large part by insurers. I sincerely hope that the Physicians who make up PROP do not agree that this is a humane, rational and responsible means of effectively treating patients.
Their contention based in citations 10 and 11, number 4 in their petition, is actually supportive of a conclusion opposite to their own. If patients on long term opioid therapy continue to experience pain, this might very well indicate that the dose they are receiving is not sufficient to completely obliterate their pain. In reality, most long term opioid patients are aware that opioids do not eliminate all pain. The expected outcome is an improvement in the quality of life. One has only to scroll down thru the posters in citation 11 to see how ludicrous it is to use this citation in support of their argument. The authors of these citations just happen to be the Physicians and researchers who comprise PROP. The basis for citation 11 are short term studies with low population and significant pre-selection. Suggestions, which is all that can be culled from this and other of their citations, are often very far reaching, highly inconclusive and unsupported by external study. This is not good science.. Not at all.
One of the doctors from this group made comment about me that was so far devoid of reality I immediately laughed, but subsequently felt a sadness that this errant thinking continues today.
Steve Gelfand, MD August 29, 2012 6:33 pm
The post by M. Dennis Paul raises the issue of the rising volume of morbidity and mortality in chronic noncancer pain patients on chronic opioids who may also have "anxiety, depression, PTSD, psychosis and multiple medication and/or alcohol abuse." But he fails to recognize that it is precisely this large segment of the chronic pain population in whom pain is directly related to the effects of chronic psychological distress acting on the central nervous system [and not to peripheral tissue-based pathology like of cancer, neuropathic pain or end-stage arthritis], which has a much higher risk for the addictive and lethal effects of opioid analgesics. These are the types of patients for whom primary care providers have for so many years overprescribed opioids for the misguided hope that opioids can "relieve pain and suffering," as encouraged by organizations like the AAPM and many others in the pro-opioid movement in the complete absence of scientific evidence.<
Dr. Gelfand's contention that “it is precisely this large segment of the chronic pain population in whom pain is directly related to the effects of chronic psychological distress acting on the central nervous system [and not to peripheral tissue-based pathology like of cancer, neuropathic pain or end-stage arthritis], which has a much higher risk for the addictive and lethal effects of opioid analgesics,” is nowhere supported in any corroborative and appropriately conducted and reviewed study. I dare say this eliminates their own studies which appear to be minimally and selectively peer reviewed. Having been a member of a clinical dual diagnosis treatment program, I can attest to the falsity of Dr. Gelfand's contention. Dr. Gelfand appears to subscribe to the old canard that says
“It is all in their head”, a perspective that marginalized client reports of pain for decades and dismissed those clients as irrational, hysterical and not worth the care and compassion afforded primarily to only chronic cancer patients.
I like to remind people that women, in particular, were defined as a disease in medical textbooks right up until the early 70's in the US. It's true. Medicine knew so little about the female body it preferred to relegate it to a state of illness. This coincided with the notion wrought in Psychology and Psychiatry that most all complaints of health issues stemming from women were presentations of “hysteria”. Even today, women are given less regard than males both in private practice and in the ER.
Not so long ago, I had to physically threaten an ER doctor to stop minimizing the concerns of my then wife and run the tests suggested by her complaints. He actually told me straight out that her presenting pain was “all in her head”. The outcome? My then wife had an embolism which, if untreated would have assuredly killed her.
Addressing the recommendations of PROP as they are listed is a rather simple matter. The 1st is:
Strike the term “moderate” from the indication for non-cancer pain .
Pain is subjective and often quite transient even in those with chronic pain. Even in those with chronic cancer pain. In my case, pain typically ranges from moderate to severe (crippling). Unless any of these petitioner's actually experiences what I and millions of others with “non-cancer” pain experience, they are completely out of bounds to propose the term “moderate” be stricken. PROP offers no scientific basis for so eliminating the term. The 2nd recommendation is:
Add a maximum daily dose, equivalent to 100 milligrams of morphine for non-cancer pain.
Again, PROP offers no valid research demonstrating the value of their proposition. Again, PROP relies on the outdated canard of “non-cancer vs. chronic cancer” as rationale for prescription and/or dosing. They completely ignore the common feature of pain treatment which is called “breakthrough” pain. Pain is not a static condition. It fluctuates and will, at times, break through the therapeutic barrier provided by a standard dose. Too, it ignores the reality that with some individuals and with some medications, effectiveness wains and can be addressed by increasing dosage to what again becomes therapeutic. Sometimes the drug fails completely and another may be implemented to regain a therapeutic hold on pain.
Sometimes no measure can effectively moderate pain for some.
Up until just a few years ago, medical students received 1 hour of pharmacology which only vaguely touched upon psychopharmacology. Graduating doctors then relied upon medical flyers, posters at conventions and pharmaceutical reps to gain what little knowledge they had regarding the medications they prescribed. To date, I have received more formal training in psychopharmacology than any of the doctors who have treated me over the years. The only doctor with whom I can intelligently converse on this subject is my personal pain management physician. Still, I continue to inform him on various medications and their interactions. Together, we investigate any and all prescribed medications and OTC remedies, vitamins, herbs, etc that I might use and I will not take anything new until we have both discussed use.
The 3rd and last recommendation from PROP is:
Add a maximum duration of 90-days for continuous (daily) use for non-cancer pain.
Once again, the inference is that only cancer patients should be allowed adequate pain relief for the duration of their disease. Once again, no valid scientific evidence exists in support of this proposal. The non-citizen petition of PROP fails to offer any supportive science, reason or rationale for their petition.
Further, it is most disingenuous to cloak support for this petition by listing names of the PROP members with the statement “Not Under US Senate Investigation” and listing AAPM Directors with the statement “Under Senate Investigation”. This is, of course, done in an attempt to castigate these individuals, in effect convicting them in a public forum prior to any formal charges having been levied against them. It is very poor journalistic style and purposely deceptive. Perhaps charges will come as will trials and findings one way or another. In the course of any year, thousands of people come under Senate investigation. Until convicted, it amounts to absolutely nothing. Too, we can look at who are the investigators and wonder why some, if not all, are not themselves under investigation for accepting influence from corporations and lobbyists and more.
Now debunked, does this mean that concerns regarding prescriptions of opioids should be cast to the side? Absolutely not. Are concerns about over prescribing valid? They certainly are... not universally, but valid none the less. Are Pharmaceutical companies without blame for greedily promoting their drugs and influencing greater use than is necessary? You bet they aren't ! That is the history and nature of pharmaceutical companies. They manufacture drugs and it is an unwritten mantra that chants “Drugs Into Bodies”. What then is the answer...or answers to the problems at hand?
First and foremost is to eliminate the emotionalism surrounding Opioids. Understand that opioids most definitely serve a valuable purpose. Get beyond any notion that they are ideal. Admit that pain is subjective and that canards such as “chronic cancer or non-cancer” pain serve no purpose. Recognize that many humans suffer from more intense and chronic pain than cancer pain. Admit that pain is subjective and has to be carefully discussed, assessed, prescribed and monitored because there is no possibility of deriving truly usable and conclusive data beyond that directly involving the individual. Redefine addiction so that it more accurately reflects the many gray areas of use and fully recognizes addiction as rooted in thought as opposed to some mechanism by which a drug selects those who will become addicted.. Get rid of the false notion that “it is all in their heads” and begin to respect the client. Understand that there may be more benefit in clinically administering Heroin to those who find it impossible to eliminate its use. Remind yourself that methadone has greater physiologically damaging characteristics than any other known opioid and is potentially more deadly. Recognize that roughly 1/3 of patients using a specific drug, any drug, will either not respond or will negatively respond to the drug. This means greater awareness on the part of prescribers and a willingness to experiment within bounds. Recognize that Oxycodone is next in line to Methadone and should be more carefully controlled and less frequently used... as should Methadone. Recognize that current and future doctors need considerably more training in pharmaceuticals than they presently receive and that they should also receive considerably more training in therapeutic pain management and prescription control. Investigate and prosecute the real pill mills... the pharmaceutical companies that dump products in more relaxed countries who then promote smuggling of those drugs into the US. Realize that there are far more painkillers on the street than are prescribed in any given year. Inform users to avoid smoking opioids from aluminum foil because some compounds within these drugs can react with aluminum causing brain injury and death.
Recognize those practices that genuinely control pain medication without withholding it or over prescribing. Educate yourself to the very real fact that over 106,000 adverse drug reaction deaths (Iatrogenic) occur each year, that 98,000 deaths from medical error (iatrogenic) occur each year, that 32,000 surgery related deaths occur each year, that 115,000 deaths occur each year from bed sores (iatrogenic), that 37, 136 unnecessary procedure deaths occur each year (iatrogenic), that 108,800 deaths occur each year from iatrogenic malnutrition, that 88,000 iatrogenic infection deaths occur each year and that 199,000 iatrogenically induced outpatient deaths occur each year...in the US. What does Iatrogenic mean? Deaths induced inadvertently by a physician or surgeon or by medical treatment or diagnostic procedure. Every year, in the US, roughly 784,000 iatrogenic deaths occur. Remember that roughly only 16,000 deaths each year are attributed, though not fully substantiated,to opioid use. Begin to put things into perspective and understand history. This will eliminate hysteria, promote clearer thinking and lend itself greatly to solving problems rationally, reasonably and effectively. Factually recognize that opioid use in the US pales in comparison to Opium use at any given time in history and that it is not the “epidemic” of which it is being promoted.
Recognize that societies throughout history who were tolerant and supportive of Opium use experienced considerably less societal degradation than is experienced in intolerant societies. Recognize that properly controlled heroin addicts are far more likely to maintain stable homes and jobs, are less prone to infection and disease, do not resort to crime and pay their taxes. Recognize that Opium is far more effective than the vast majority of the drugs derived either directly from isolation or synthesized, can honestly be claimed to cause fewer deaths, is cheaper to produce, easier to cease use, and a hell of a lot more pleasurable in the long run (even more so than heroin, which many might disagree). Recognize that Marijuana is a highly effective pain medication, has absolutely no recorded history of deaths, works compatibly with Opium for maximum effect from minimum dose, is inexpensive to produce and cannot be honestly promoted as an addictive substance.
Two anecdotes: As a young man living in Boston, I had call to present to the Mass General Hospital whereupon I was given a prescription for a pain killer. I went into the hospital’s pharmacy and discovered to very well done tiled pictures which framed the pharmacy's window. On one side was a large picture of the Opium Poppy and on the other was a large picture of the Cannabis Plant. Not being one to shy away from asking questions, impertinent or not, I asked the Pharmacist howit came to be that these pictures adorned the pharmacy walls. In a sweeping gesture, he presented the row upon row of bottles containing hundreds of various medications, looked me straight in the eyes and stated, ” If we were allowed to dispense these two medications, legally, we would have virtually no need for 99% of all the bottles you see here. History tells us this is the truth. My professor, long an associate of the pharmaceutical industry, will attest otherwise...but with a sly wink.”
Working in drug rehabs over a number of years, there was a sudden influx of clients claiming they had come to “kick” their marijuana addiction. In each and every case, when asked when they firs realized they were addicted to pot, they responded, “When the judge told me I would have to spend 6 months to a year in jail or go to a drug rehab for 28 days.” When asked if they were experiencing withdrawal symptoms, the common response was a puzzled expression, an “I'm not sure”, and “Well, I wouldn't mind sparking one!”.
Hence, the erroneous construct of Marijuana addiction.
One other recommendation I would like to make here (I suggest there are other rational and reasonable recommendations which other might add) is that the US government recognize, legalize and begin training therapists in the use of the most effective medication yet discovered to safely and effectively both assist in detoxing drug “addicts” (including “alcoholics”) and assisting them to psychologically address past traumas and present cognitive distortion which are, in fact, the root of all addictions. This plant is called Iboga and its extract, Ibogaine, is technically an hallucinogenic. The literature on this medication, along with the first hand exposure I have had with many who have been treated with it, strongly calls for it to be legalized and its use implemented post haste. I firmly believe that if made available, more mothers and others will be saved from having to bury their children, friends, parents, or whomever. Ibogaine info can be found here: www.ibogaine.desk.nl
To PROP and followers: If you want to truly be an organization of change, cease polarization and witch hunts, poorly constructed research ill used to legislate irrational control of medicine, study history and stand out front for legalization, clinical application, tolerance and rational, humane treatment. Otherwise, you are just one more problem in the way of same. The same applies to AAPM and any other group.
This author states that he is not in the pocket of any corporation or egocentric control promoting organization nor is he a proponent of genuinely deplorable “Publish or Perish” “science”.
 M. Dennis Paul, Ph.D. is a Counselor and Conflict Resolution Specialist/Consultant (Mediation/Arbitration/Facilitation) (20+ yrs).
M. Dennis Paul, Ph.D. is a Counselor and Conflict Resolution Specialist/Consultant (Mediation/Arbitration/Facilitation) (20+ yrs).
He is the Creator of Thought Addiction programs (Lectures Seminars & Workshops) (Intensive 21 day Addiction Recovery Programs designed for Artists, Actors, Musicians & Industry Leaders) residing in New Hampshire (US). (The Website for M. Dennis Paul, Ph.D. is currently under reconstruction) Contact: mdp54@gsinet.net 1-603-478-1544
 |
 |
 |
 |
 |
 |
 |
Articles for September 7, 2012 | Articles for September 8, 2012 | Articles for September 9, 2012
Quick Links
DINING
Willamette UniversityGoudy Commons Cafe
Dine on the Queen
Willamette Queen Sternwheeler
MUST SEE SALEM
Oregon Capitol ToursCapitol History Gateway
Willamette River Ride
Willamette Queen Sternwheeler
Historic Home Tours:
Deepwood Museum
The Bush House
Gaiety Hollow Garden
AUCTIONS - APPRAISALS
Auction Masters & AppraisalsCONSTRUCTION SERVICES
Roofing and ContractingSheridan, Ore.
ONLINE SHOPPING
Special Occasion DressesAdvertise with Salem-News
Contact:AdSales@Salem-News.com


Terms of Service | Privacy Policy
All comments and messages are approved by people and self promotional links or unacceptable comments are denied.
gp September 9, 2012 1:14 pm (Pacific time)
Brilliant! I would only add to your list of drugs that would make others unnecessary the miracle, DMSO also maligned by the medical establishment.
[Return to Top]©2026 Salem-News.com. All opinions expressed in this article are those of the author and do not necessarily reflect those of Salem-News.com.